

Is That Blood?
Cutting. It’s a scary moment for even the most seasoned parent. Maybe you noticed some scratches on your daughter’s arm before. At that time you simply dismissed it as “nothing” or she explained it away by saying the family cat had scratched her. But now you’re seeing it again and your heart is telling you something is wrong.
Maybe it’s something else. You’ve noticed some bloody tissues in the bathroom on a few occasions. Your kid has stopped going to the beach or the pool when they have always loved doing so. Or better yet, it’s 80 degrees out but your daughter is still wearing long sleeved shirts which she explains is the latest fashion. It’s probably not and the better part of you knows that. But you don’t know what to say, what to do…
This is a mental health disorder known as Self Harm or Self Injury. It can take many forms from intentional cutting to cigarette burns, scratching, biting, carving, pinching of the skin, hair pulling, or literally banging their head against a wall. Cutting typically takes place on the arms, legs, or stomach. If not addressed quickly it can turn into a very difficult habit to break.
Since the Covid pandemic the prevalence of self harm among teens has increased dramatically. Self harm typically starts in pre-teen to early adolescence but can start earlier or occur later in life. While typically impacting teenaged girls, boys are also significantly impacted by this phenomenon as well. It can last for days, weeks, months, or years. More cyclical than linear, it may come and go. Recovery can also be a process, be non-linear, and take some time.
Is My Teen Attempting Suicide?
Seeing cuts and scratches across your daughter’s wrists can immediately draw upon your worst fears – my kid is trying to end her life! However, this self-harm does not necessarily mean this is an attempt at suicide. The differentiators include whether or not your teens’ intention while inflicting the self-harm was to end their life or not and how they feel the self-harm serves them.
If the intention of the teen was to die then it is a suicide attempt. When their intention is not to end their life this is known as Non Suicidal Self Injury (NSSI). The International Society for the Study of Self Injury defines NSSI as, “The deliberate, self inflicted destruction of the body tissue resulting in immediate damage, without suicidal intent and for purposes not culturally sanctioned.” (ISSS, 2007).
While NSSI is not a suicide attempt there are some correlations that are concerning. 70% of teens that are involved in NSSI will make at least one suicide attempt in their lives. 55% will make multiple attempts. According to the National Institute of Health this self-harm is the highest risk factor and is often among the other risk factors for suicide including depression, anxiety, and borderline personality disorder. Getting accustomed to hurting oneself can make it easier to attempt suicide due to the desensitization of pain associated with self injury.
Why Is My Teen Cutting?
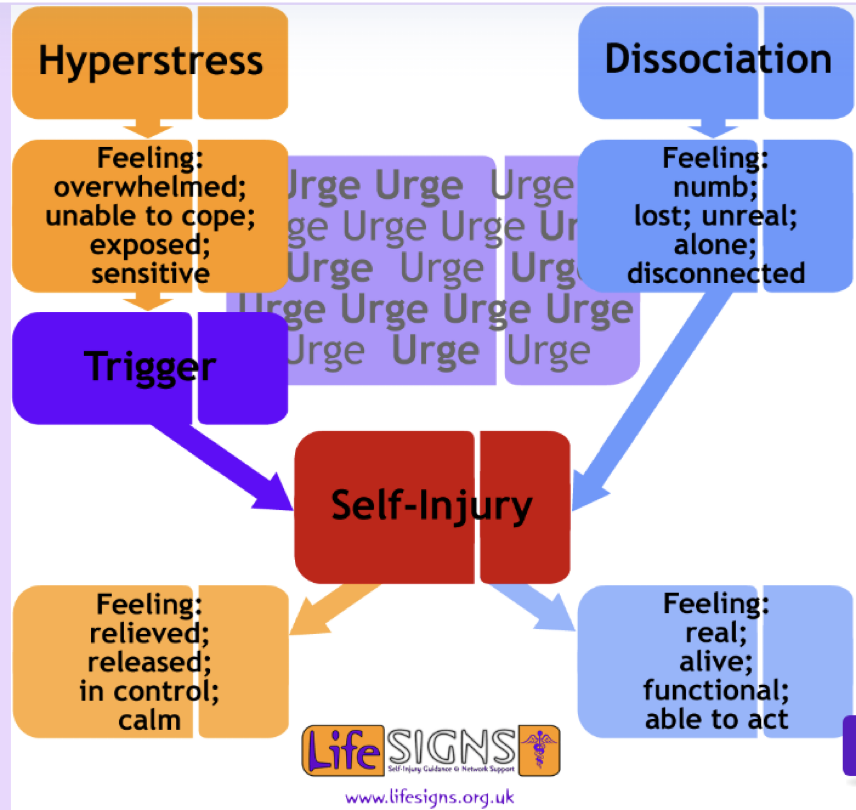
So, if it’s not suicide why is my kid doing this? The world-renowned resource on NSSI, Michael Hollander sums it up best in that, “self injury is a means to end emotional suffering.” Teens who are self-harming are essentially overwhelmed by and have extreme difficulty managing intense emotions. For them cutting is a way of getting themselves emotionally regulated again. It is a learned, yet temporary and dysfunctional coping mechanism. Kids who use NSSI are typically driven by one of two reasons – hyper stress or disassociation.
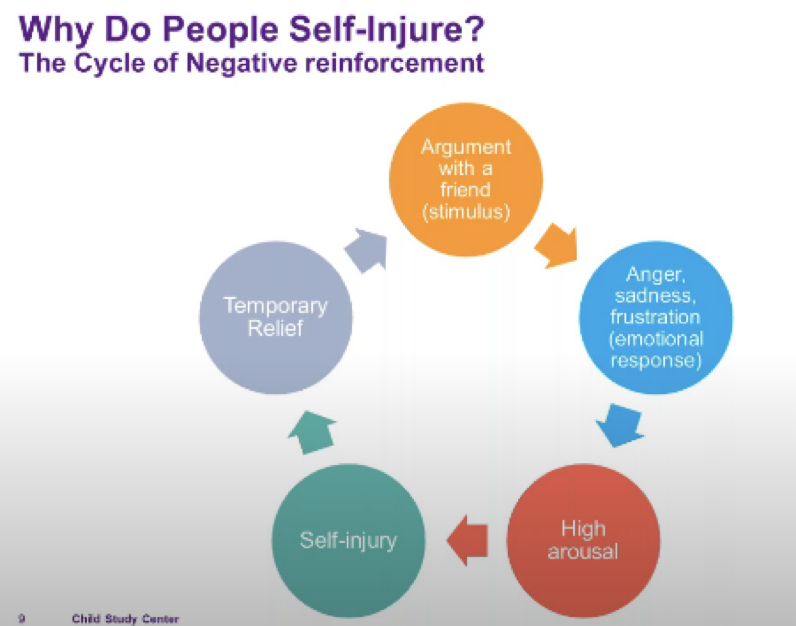
Hyper stress describes this feeling of being overwhelmed and unable to handle a wave of emotions. The teen is flooded and things feel out of control. Without a means of understanding what is happening for them or how to regulate the feelings they resort to self harm. The cutting provides relief from these out of control feelings and helps them to feel relieved, in control, calm, and better. This psychological process, known as Automatic Negative Reinforcement provides relief through a phenomena called Pain Offset Theory where through self injury you start to feel calmer than you did before. The problem is that it is only temporary and leads to a dysfunctional cycle where the process is repeated without resolution.
For others NSSI provides relief from a period of dissociation where there is an inability to feel anything, a sense of numbness, disconnectedness, loss, or a feeling that things are unreal. This group derives their relief through self harm in a process known as Automatic Positive Reinforcement. Here the cutting helps them to reconnect, feel alive, and real again.
Many of the teens I’ve worked with who were struggling with NSSI have fallen into these two groups.
A 16 year old girl told me:
- “It helps me to express something I can’t say”
- “I start cutting because it doesn’t feel like stuff is happening. I don’t feel real. It brings me back to the moment.”
- ”It’s a way to express myself. Other people can see what I’m feeling without me having to say it. It feels awkward to say it out loud like, “I’m depressed. I’m going through some stuff.” “
- “It would be nice if someone saw it and asked, “Are you okay?” “
A 15 year old girl said:
- “I get overwhelmed from my fear of abandonment. Like everyone in my life is going to leave me like my mom did.”
- “It happens if I have a fight with my boyfriend, he breaks up with me, or my classmates bother me.”
- “I can’t take it and cutting helps me, like to let the tension go.”
- “Most of the time I don’t even remember what I was thinking or feeling before. I just know when my arm starts to feel sore.”
A 14 year old boy said:
- “Cutting helps me to stop thinking about things that mad me mad.”
- “Sometimes I think things are all my fault and I don’t know what to do”
How Do We Talk About It?
When you first come to realize your teen is engaging in NSSI you are bound to be filled with any number of emotions. You might feel angry, disappointed, scared, disgusted, embarrassed, anxious, sad, and more. All of this is common and normal. You may also feel a sense of guilt. As if you dropped the ball while parenting. Give yourself a moment to breathe and grant yourself some grace – this isn’t likely because you were a bad parent. Allow yourself to work through your feelings before you try to talk about this with your teen. Just like when you are boarding an airplane and the flight attendant tells you about the oxygen masks that may drop out of the ceiling – Put your mask on first before you try to put a mask on your child.
By listening to what your body is telling you what you are feeling, allowing those emotions to happen, and labeling them you will be demonstrating for yourself the emotional regulation that your child is lacking. You are “surfing” the emotion. Take note as it is in this kind of moment that you are not cutting, but your kid is.
Once you are in a good emotional space find a good time and place to talk with your teen. You’ll want a place that is quiet with no distractions. Sit next to them rather than across from them. Approach the topic with warmth, compassion, unconditional positive regard, and a gentle sense of curiosity. Chances are your teen has been hiding this and they are going to have an emotional response to you brining this up. Go slow. Your patience in this moment will help to you to gain their trust. Use your own words but along the lines of, “I wanted to let you know that I’ve seen the cuts on your arms. [Pause] It has me worried about you. [Pause] I’ve learned that cutting has different meanings for different kids. Can we talk a bit about this and maybe you can tell me how it helps you, what it means for you?”
Your kid may not be willing or able to talk with you about this right away. Let them know that that is okay. It will take some time for the knowledge that you are aware now to settle in with them. You can offer to continue the conversation later, give them a choice as to when and where, or even allow them to chat with you about it through text which for some is an easier way to begin the dialogue.
Avoid making this conversation into a confrontation. Doing so will almost certainly make things worse and can lead to their self harm going “underground” where they may cut in places that are harder for you to find. You’ll then need to start over and work to rebuild their trust. If the conversation isn’t going well for either of you take a break and come back to it at a later time.
As you have the conversation with them let them know that you want to get them some professional help to manage this. Let them know that many other kids have and are going through the same thing and that there is professional help available that can help them to gain control and mastery over this. Let them know you care and love them and that you’ll be there for whatever role you can play to help them with this.
Parent Dos and Don’ts
Dos:
- Check your emotions first. Give yourself some time.
- Find the first available time you can to bring this up. As soon as is feasible though not ASAP
- Stay neutral and open
- Validate what your child tells you. Give feedback and get confirmation that you understand them. *
- Listen with compassion
- Accept them
- Share with them that what you’ve learned is that cutting helps them in the moment but that it doesn’t solve the issues that led them to cut in the first place
- Include them in getting professional help. This will help build a sense of autonomy and control
Don’ts:
- Don’t punish them, get angry, yell, panic, or overreact
- Don’t threaten or criticize
- Don’t demand answers or make ultimatums
- Don’t lecture or threat
- Don’t ask them to recall all of the details of the self harm behavior
- Don’t monitor your kids self injury.
- Don’t engage in body checking
- Don’t attempt to remove every sharp object from the house.**
* – Validation helps them to get in touch with what they are feeling. Provide feedback and get validation that you understand what they are feeling and what is triggering it. Doing this with your kid will help them in a critical step toward their mastery over this behavior.
** – In NSSI your kid will find more sharp things than you can hope to hide. More importantly, your kid will work to do their self harm in more covert ways and the level of mistrust between you will be high if you try to hide all sharps. Ultimately you want your child to be able to live in a world where sharp objects exist but they no longer make a choice to use them in dysfunctional ways. (Note – For suicidal ideation it is strongly recommended to remove all items that can be used to end their life.)
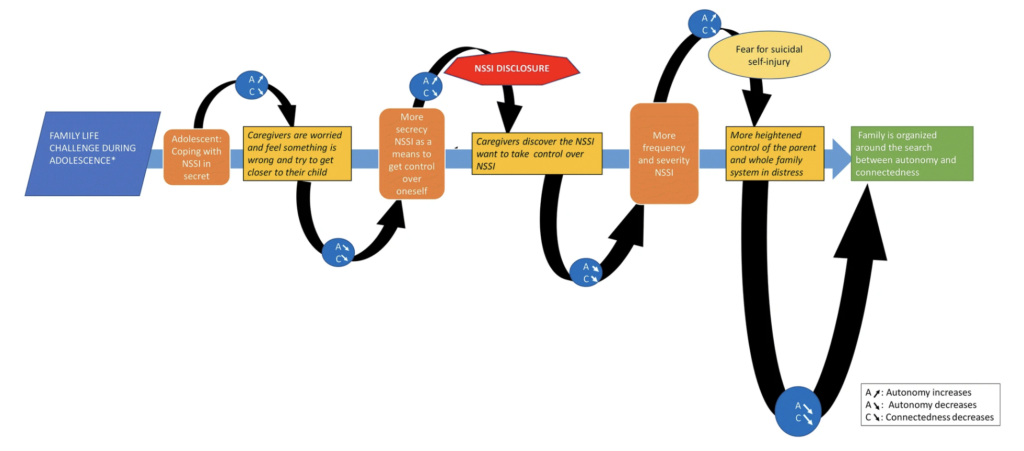
Effectively helping your teen with NSSI involves a careful balance between your connectedness with them and their sense of autonomy:
Therapy That Works
It’s important to seek professional help as soon as possible. The longer NSSI continues to be used as their coping mechanism, the harder it can be to break away from. However, it is important to select a therapist who has experience working with adolescents and NSSI. Evidenced based therapy methodologies are guided by scientific evidence and research and provide the best treatment options for teens who are self harming. Two such therapy methodologies include Solution Focused Brief Therapy (SFBT) and Dialectical Behavioral Therapy (DBT).
SFBTs focus on developing strengths, eliciting exceptions, and future directed approach to developing solutions lends itself well to NSSI clients. North East Yorkshire NHS Trust performed a study on the effect of SFBT on 40 NSSI clients. Of the 40 only one repeated self harming in a six month follow up period. A critical factor in the success of SFBT with this population was the ability to work together with the client to form well defined treatment goals as well as the criteria which would determine successful achievement of those goals. Developing and encouraging the clients sense of autonomy empowered them to gain mastery over the self harm. An emphasis on envisioning their lives after the problem of self harm had been resolved allowed them to develop their own set of competencies and skills.
DBT is an evolution of Cognitive Behavioral Therapy (CBT) that has extensive emphasis on helping clients to manage intense emotions, learn ways of regulating them, and identifying and changing negative thought patterns. It is a comprehensive approach that can include a combination of individual therapy, family skills groups, phone coaching, and a DBT consultation team for the therapist. One skill of DBT, Mindfulness of Current Emotions, is an emotional regulation strategy that helps clients to observe and accept emotions without judgment. This ability to become more aware of and accepting of ones emotions can help teens struggling with NSSI from hyper stress learn to regulate and manage their emotions, reducing the probability of being overwhelmed by them and resorting to cutting as a means of release.
If you or your child are struggling with NSSI, suicidal thoughts, or managing their emotions the team at Kellen Mental Health have experienced and skilled adolescent therapist ready and able to help you navigate these waters to a future without self harm.
Book Recommendations:
- Stopping the Pain: A Workbook for Teens Who Cut and Self Injure by Lawrence E. Shapiro, PhD
- Helping Teens Who Cut: Using DBT Skills to End Self-Injury by Michael Hollander
- Holy Sh*t, My Kid is Cutting! By JJ Kelly, PsyD
Online Resources:
- 1 – Life Signs – https://www.lifesigns.org.uk/
- Understanding Self Harm in Children/Adolescents – An online workshop video for parents and caretakers of children managing NSSI – https://www.youtube.com/watch?v=CJVd8lVXFHw
References
- Nonsuicidal Self Injury in Adolescents – Peterson, Feedenthal, Sheldon, Andersen 2008
- A Solution-Focused Approach to Working with Clients Who Are Suicidal – Sharry, Darmody and Madden 2002
- SFBT with Self Harm – Farist 2016
- Strategies to Deal with Suicide and Non-Suicidal Self Injury in Borderline Personality Disorder, the Case of DBT – Prada P, Perroud N, Rüfenacht E, Nicastro R. Front Psychol. 2018 Dec 17;9:2595. doi: 10.3389/fpsyg.2018.02595. PMID: 30619004; PMCID: PMC6304419.
- Solution Focused Approaches for Treating Self-Injurious Thoughts and Behaviors Jerome L, Masood S, Henden J, Bird V, Ougrin D. BMC Psychiatry. 2024 Oct 1;24(1):646. doi: 10.1186/s12888-024-06101-7. PMID: 39354404; PMCID: PMC11443805.
- 2- Trauma nursing 5: Identifying and Assessing Patients Who Self Harm – Da Sliva Miranda and Samy 2023
- 3- The NSSI Family Distress Cascade Theory – Waals, Baetens, Rober, Lesis, Parys, Goethals and Whitlock 2018
